
Home births are being talked about more as a safe space in the setting of startling Maternal Mortality numbers in the U.S. Meghan Markle recently gave birth and a flurry of news articles and blog posts followed. This one caught my eye.
Apparently Meghan Markle Wasn’t Able To Give Birth At Home Like She Planned

The article highlighted three parts of the royal birth story.
- Meghan Markle, who gave birth Monday, apparently had to change her birth plan at the last minute.
- Meghan, who planned on giving birth at home, was “whisked off” to a hospital.
- Recently, top ob-gyns at the annual meeting of the American College of Obstetricians and Gynecologists poked fun at Meghan’s home-birth plan.
I reposted the article without comment, just to see what people would say. There was a fair amount of support around her desire to avoid the hospital setting where her skin color could make her less safe. It is no secret that the black maternal morbidity and mortality rates in the U.S. are disturbing. Articles like this one highlight the concerns with hospital births:
Black Moms Are Loving Home Births
This article points out the fact that:
“According to the CDC, black mothers in the U.S. die at three to four times the rate of white mothers, one of the widest of all racial disparities in women’s health.”

As a result, more and more African American women are turning to home births to avoid the risks and disparities related to birth. They are trading the fear and distrust of hospitals for the comfort and security of home, putting trust in their own bodies to navigate the birth of their children.
The mortality rates of black women are jarring. An article from NPR that referenced the CDC stats put the numbers in a stirring perspective.
A black woman is 22 percent more likely to die from heart disease than a white woman, 71 percent more likely to perish from cervical cancer, but 243 percent more likely to die from pregnancy- or childbirth-related causes.
You don’t have to be a black woman to find those stats disturbing. But I am a black woman. I can’t help but relate to the fear and anxiety that numbers like this cause.
But in addition to being a black woman, I am fortunate to be one of the 2% of Black Female Physicans in the US.

Looking through my medical doctorate lens, I need to point out some of the flaws in using the black maternal mortality rate to justify home births.
First, let’s examine what these women are dying from.
According the Center for Disease Control, and looking at the years 2011-2014, the most common causes of death were as follows:
- Cardiovascular diseases (Heart disease), 15.2%.
- Non-cardiovascular diseases (like Diabetes), 14.7%.
- Infection or sepsis, 12.8%.
- Hemorrhage (Excessive blood loss), 11.5%.
- Cardiomyopathy (Heart malfunction), 10.3%.
- Thrombotic pulmonary embolism (Blood clot), 9.1%.
- Cerebrovascular accidents (aka Stroke), 7.4%.
- Hypertensive disorders of pregnancy, 6.8%.
- Amniotic fluid embolism (It’s like a clot), 5.5%.
- Anesthesia complications, 0.3%.
Of those, the only one that is directly related to being IN the hospital is the anesthesia complication risk.
Another article from the National Institute of Health looked at “national data sets to calculate prevalence and case-fatality rates among Black and White women for the years 1988 to 1999.” Though it did find that black women were 2-3 times more likely to die than white women, the causes of death were the following:
- Preeclampsia
- Eclampsia
- Abruptio placentae
- Placenta previa
- Postpartum hemorrhage
Again, terrible and tragic, but not related to being IN a hospital vs outside of one. Preeclampsia, for example, is a syndrome that causes high blood pressure and organ function abnormalities but is caused by the pregnancy. African American women are more likely to develop this condition, as are women with pre-existing high blood pressure, diabetes, and who are overweight.
I propose that women who are considering home birth look at these stats through a lens of cause vs treatment. Did the hospital, doctor or nurse cause the life-threatening disorder, or did the lack or proper or prompt treatment lead to the loss of life? Logic tells me that if these disorders were not caused by the healthcare system, the latter must be true. Being at home would not lessen that risk, it would increase it.

Serena Williams spoke to Vogue magazine about her difficultly in receiving prompt evaluation and treatment for the blood clot that almost killed her. And there is the chilling story of Kira Johnson, a mother of one who died 12 hours after the birth of her second son due to hemorrhage because the hospital and healthcare providers delayed evaluation and treatment until it was too late.
The problem, as I see it, is a deficiency in recognizing the diagnosis and lack of appropriate treatment. It is passive neglect, not active harm.
The solution lies in addressing biases, and establishing protocols that react to objective findings rather than subjective ones. At my hospital, blood loss volume and vital sign abnormalities immediately set off a cascade of protocols, quickly involving the doctors and nurses from the OB and anesthesia teams.
Concrete, objective criteria to rapidly initiate care also eliminate racial and socio-economic biases because they are strictly based on the numbers. For example, every patient at my hospital has vitals checked every 15 minutes initially after birth. Everyone has a bleeding check every 15 minutes as well. Failure to follow these protocols and strictly document them can result in severe remediation of any and all healthcare providers. Following the rules is not optional, it is required if you want to keep your job.
But Doc, I worry that a hospital is going to make my birth experience an unpleasant one.
Addressing some of the concerns with hospital births feeling sterile or emotionless,
There have been many advances in the obstetric community in the last decade or so that encourage less intervention and more flexibility when it comes to monitoring labor progress. In my own career, the definition of stalled labor has changed dramatically. We only offer intervention when necessary.
Even the definition of “normal labor” as it relates to how long progress is taking has changed immensely. And, while I can’t speak for all OBGYNs, at least at my hospital midwifes and doulas have positive relationships with OBGYNs, rather than antagonistic ones. Women are often surprised at how calm labor and delivery can be. Pushing can come in many forms and options. Women can often walk and even shower during labor. But when intervention is needed for the safety of mom and/or baby, we are there.
In the United Kingdom,
… home births are often attended by a midwife. In the US, this is less often the case. At least when cared for by a Certified Nurse Midwife, problems can be recognized quickly. Emergencies are still not always easy to manage, but at least treatment can be expedited.

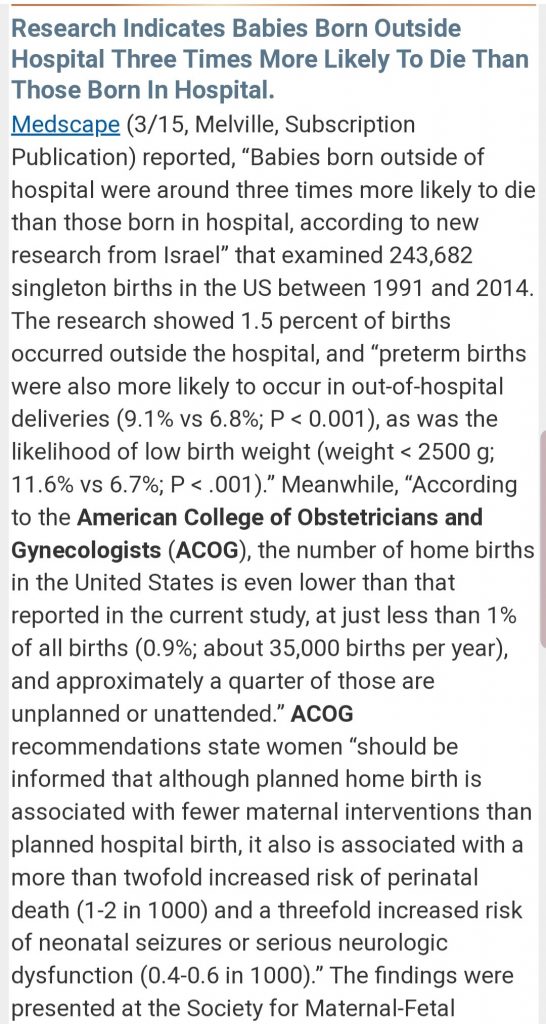
And even though we all know women, or know of women who have delivered safely at home, that doesn’t eliminate the risks to mom and baby in the U.S., and abroad. The article below talks about the mortality rate of babies born at home in Israel. Babies were 3 times more likely to die when born at home versus the hospital.
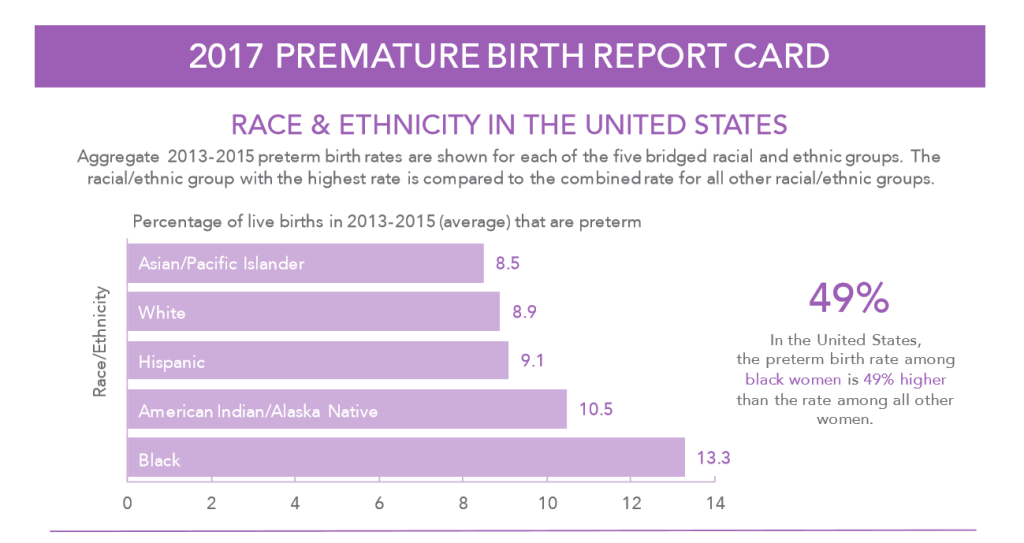
And prematurity rates are higher among African American women. According to the march of dimes, more than 13% of African American babies were born preterm, or early, which also increases their risk of harm and death rates. Home is absolutely not the place to have these babies.
This decision isn’t like choosing home school because the school system is failing your child. Taking education into your own hands can definitely improve outcomes in certain circumstances. This is more like having a dentist who doesn’t find and fix all of your cavities. The solution isn’t to avoid dentists all together. Hygiene alone won’t necessarily save you, especially if you are predisposed to cavities (like me.) You need a better, more meticulous dentist.

Ultimately, ALL women want a safe and healthy delivery of their sweet baby. Women also want the experience to be beautiful and full of love, not fear and anxiety. I appreciate that concern, but my own personal experiences won’t let me ignore the risks. In my own pregnancies I had preeclampsia with one of my babies, which threatened my life, and cholestasis of pregnancy with another which threatened my babies life. My birth experience could have ended tragically if not for my hospital births.

I encourage ANYONE considering a home birth to reconsider.
Instead find a trusted provider, whether it be a midwife or OBGYN to attend your delivery in a safe place that is equipped for handling any emergencies that could arise. Talk to your provider(s) about your fears and concerns. Ask them about their practices and protocols. Stay in tune with your own signs and symptoms and share them, repeatedly if necessary.
In pregnancy and delivery, risks abound. Being outside of the hospital doesn’t make anyone MORE safe. Complications can arise anywhere. We as healthcare providers need work to make the hospitals themselves more equipped to rapidly handle those complications in a standardized way.
Just my thoughts. Blessings in your delivery.
